

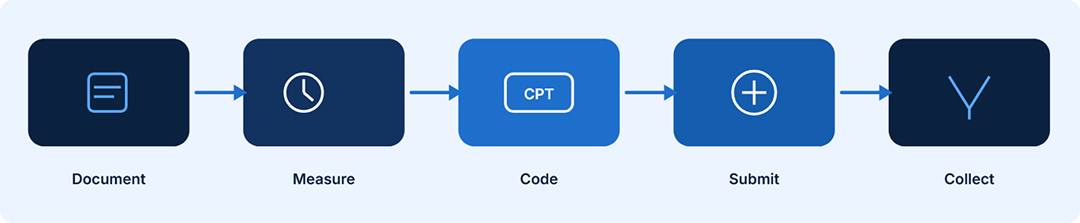
Wound care practices that master documentation and coding are consistently reimbursed faster and at higher rates than those that treat billing as an afterthought. This guide walks you through every step so nothing falls through the cracks.
Wound care is one of the most documentation-intensive specialties in medicine. Whether you run a dedicated wound clinic, a home health agency, or manage wound patients within a broader practice, getting paid correctly depends on how well your team understands coding, documentation, and payer rules.
Many practices leave significant revenue on the table every year because the right CPT code was not selected, wound measurements were not recorded, or debridement was not separated from evaluation and management services. This guide breaks down every part of the reimbursement process so your team can follow a clear, repeatable path from patient visit to paid claim. It connects directly to our broader Revenue Cycle Management approach and our Medical Billing Guides for other specialties.
End-to-end billing optimization →
Reduce no-shows, improve collections →
Most medical specialties revolve around evaluation and management (E&M) codes. Wound care is unique because it combines E&M services, procedure-specific codes for debridement, and supply codes for dressings and devices. Each carries its own documentation requirements and payer rules.
Wound care also spans multiple care settings including outpatient clinics, skilled nursing facilities, home health environments, and hospital outpatient departments. Reimbursement rates, allowable codes, and the responsible biller can all differ by setting, which makes knowing your environment essential before you code anything.
Every wound note should include wound location, size in centimeters (length, width, and depth), wound bed characteristics, exudate type and amount, periwound skin condition, and the stage or classification. Without this information, payers have grounds to deny claims for lack of medical necessity, and auditors can recoup payments even years after the fact.
Wound measurements are not optional. They drive CPT code selection for debridement and support medical necessity for ongoing treatment. Length and width should be recorded in centimeters. Depth must be included when debridement is performed. A wound that is not measured is a wound that will not be properly reimbursed.
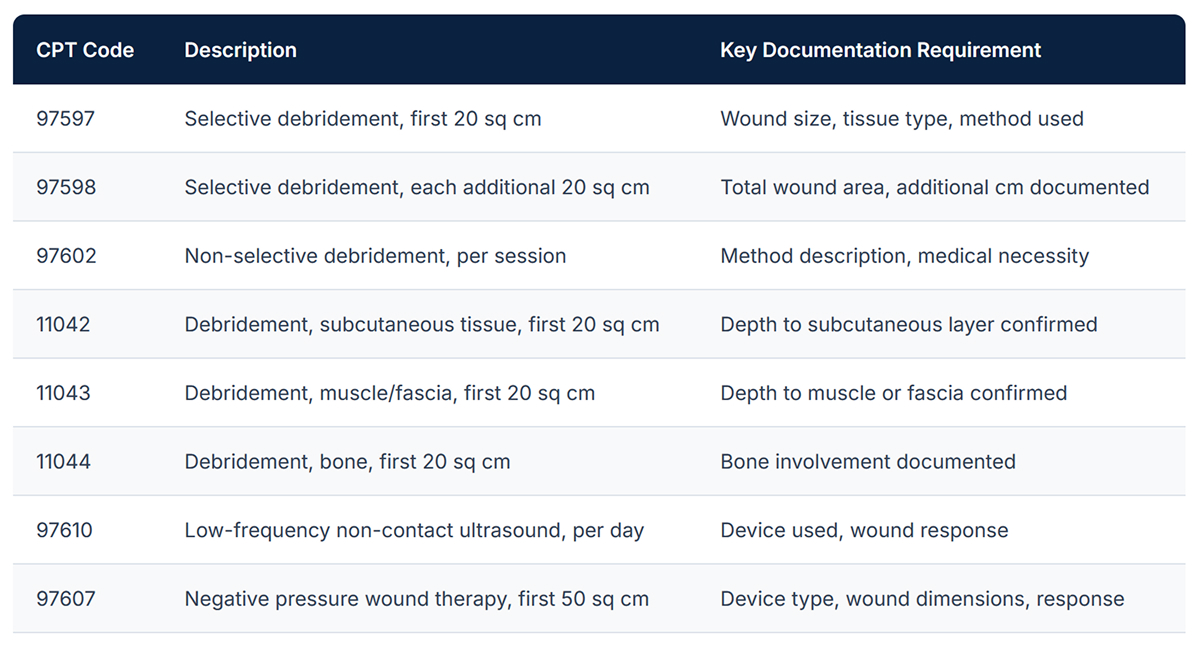
Debridement is where the majority of wound care revenue is generated. The correct CPT code depends on the tissue type debrided and the total wound surface area. Selective debridement and non-selective debridement are coded differently. Coding below the actual service level means lost revenue. Coding above it creates audit risk.
When a clinician performs a significant and separately identifiable evaluation and management service on the same day as a procedure, that E&M service can be billed in addition to the procedure code using modifier 25. The documentation must clearly support both the procedure and the E&M service as distinct encounters with their own medical decision-making.
Advanced wound dressings such as alginate, foam, hydrocolloid, collagen, and negative pressure wound therapy are billable separately using HCPCS Level II codes. Many practices either miss these charges or apply incorrect units. Each payer has specific quantity limits and coverage criteria, so understanding your payer mix is critical before billing supplies.
Medicare, Medicaid, and commercial payers often have different rules about which wound care services require authorization, how frequently debridement can be performed, and which advanced therapies are covered. Checking these requirements before the service is delivered is far more efficient than chasing denials after the fact.
A clean claim includes the correct diagnosis codes, properly linked procedure codes, provider and facility identifiers, place of service codes, and any required modifiers. Missing or incorrect information at this stage is the number one reason claims are rejected or denied before they are even reviewed for medical necessity.
Even well-coded, properly documented claims sometimes end up in limbo. Establish a systematic process for tracking claims at 30, 60, and 90 days. Denied claims should be reviewed, corrected, and resubmitted promptly. Many practices let denials expire simply because there is no structured follow-up process in place. Our Audit and Aging Claims service specializes in recovering these lost dollars.
The table below covers the most frequently used wound care procedure codes. Rates shown are approximate Medicare rates and will vary by geography and payer.
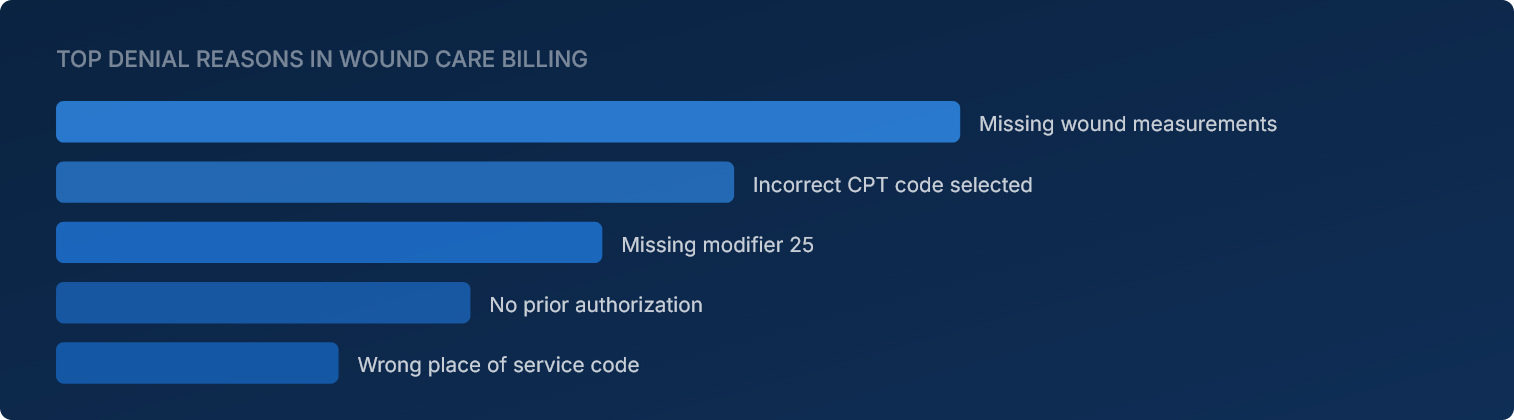
A wound without recorded dimensions cannot be coded correctly. Missing measurements are the top reason wound care debridement claims are denied or downcoded.
Practices that only bill E&M codes during wound visits are leaving procedure revenue uncaptured. Debridement, applications, and advanced therapies all have their own codes.
If the documentation does not specifically describe what was done, why it was done, and the wound's current state, payers can deny the claim on medical necessity grounds alone.
Advanced wound dressings and devices are reimbursable but only when billed using correct HCPCS codes with accurate quantities and matched to the right diagnosis codes.
Diagnosis coding in wound care must be specific to be reimbursable. A code like L89.90 (pressure ulcer of unspecified site) will often be accepted, but more specific codes that include the anatomical site and stage will better support medical necessity and reduce audit risk.
For diabetic wound patients, the underlying diabetes diagnosis must be included as a secondary code and linked correctly to the wound. For venous leg ulcers, include the underlying venous insufficiency diagnosis. Payers want to see a clear clinical story in the codes you submit, not just the wound itself in isolation.
Important: When billing for wound care under Medicare Part B in a hospital outpatient department or provider-based wound clinic, the facility and the physician may each file a separate claim. The physician bills under the professional fee schedule and the facility bills under the outpatient prospective payment system. Both sets of codes need to be accurate and the documentation must support both claims independently.
Cellular and tissue-based products (CTPs), commonly called skin substitutes, represent one of the highest-revenue areas in wound care and one of the most closely scrutinized by payers. These products have specific coverage policies, frequency limitations, and documentation requirements that vary by payer.
Before applying a skin substitute, verify that the wound meets the clinical criteria defined in the payer's local coverage determination (LCD). Document that conventional wound care was tried and failed, note the wound chronicity, and confirm that the product is on the approved product list for that payer. Submit with the correct HCPCS code for the specific product and include invoice documentation where required.
Wound care billing is specialized enough that many practices benefit significantly from working with a billing team that focuses on this area. A qualified billing partner understands the local coverage determinations that affect your payer mix, stays current with coding changes, manages prior authorization workflows, and monitors denial trends so that recurring issues are addressed at the root cause rather than one claim at a time.
At Meddabster, our team works with wound care providers across outpatient, facility, and home health settings to improve clean claim rates, reduce days in accounts receivable, and recover revenue from denied claims that might otherwise go uncollected. We handle the billing complexity so your clinical team can stay focused on patient care. Learn more about our full Revenue Cycle Management services and how we support practices like yours.
A. CPT 97597 is used for selective debridement performed by a healthcare professional using instruments, and it is typically billed when the tissue removed is limited to the wound surface area without extending into deeper tissue layers. CPT 11042, on the other hand, is used when debridement extends down into the subcutaneous tissue layer. The key distinction is tissue depth. Using 97597 when debridement actually reached subcutaneous tissue is an undercoding error that reduces reimbursement. Using 11042 when the debridement was superficial creates audit risk.
A. Yes, in most cases you can bill both, but the E&M service must be significant and separately identifiable from the procedure itself. You must append modifier 25 to the E&M code to indicate that it is a distinct service. Your documentation must clearly show the evaluation that took place separately from the debridement, including the history, examination, and medical decision-making involved in that E&M encounter. Payers will scrutinize these claims, so the documentation needs to hold up on its own.
A. Medicare covers negative pressure wound therapy in the home, outpatient, and inpatient settings, but coverage criteria and billing pathways differ by setting. In the home setting, NPWT equipment may be billed as durable medical equipment under Part B. In hospital outpatient departments, it is billed using procedure codes. The wound must meet Medicare's criteria for NPWT coverage, which include wound type, failure to respond to conventional treatment, and absence of certain contraindications. Prior authorization requirements also vary by payer, so always verify before initiating therapy.
A. Medicare has the authority to audit and recoup claims going back three years from the date of payment under normal circumstances, and up to six years in cases where there is evidence of fraud or intentional misrepresentation. Recovery Audit Contractors (RACs) and Zone Program Integrity Contractors (ZPICs) regularly target wound care providers because of the high dollar value of claims and the complexity of documentation requirements. Maintaining thorough, contemporaneous clinical records for every wound visit is essential protection against audit findings.
A. To bill for a skin substitute, your documentation should include the wound's duration and chronicity demonstrating that it has not responded to conventional care, wound measurements and clinical description at the time of application, the specific product name and the HCPCS code assigned to that product, the number of units applied, and the clinical rationale for choosing this treatment approach. Many payers also require proof of purchase or an invoice for the product. Check the applicable local coverage determination for your payer, as requirements can differ meaningfully between Medicare Administrative Contractors.
A. Medical necessity denials in wound care usually come down to documentation that does not tell a clear enough story. Even if the care was absolutely appropriate from a clinical standpoint, the payer's reviewers are reading your notes to determine whether your documentation supports the service billed. Common gaps include missing wound measurements, no documentation of prior treatments and their outcomes, vague descriptions of wound appearance, absence of a clearly stated treatment plan, and missing or incorrectly linked diagnosis codes. Reviewing your note templates against local coverage determination criteria is often the fastest way to identify where the gaps are.





.png)
